Wolf-Hirschhorn syndrome (WHS) is microdeletion syndrome characterized by a combination of distinctive external features, congenital malformations, severe developmental delay and short stature. It is caused by differently sized deletions of the terminal short arm of chromosome 4 (4p16.3), with smaller deletions correlating with milder symptoms and larger ones with more severe manifestations.
Also called
WHS is also known as:
- 4p deletion syndrome
- 4p- syndrome
- WHS
- Chromosome 4p deletion syndrome
- Chromosome 4p monosomy
- Del(4p) syndrome
- Monosomy 4p
- Partial monosomy 4p
Symptoms
WHS is characterized by a combination of distinctive external features, congenital malformations, severe developmental delay and short stature. Approximately 80% of patients have seizures.
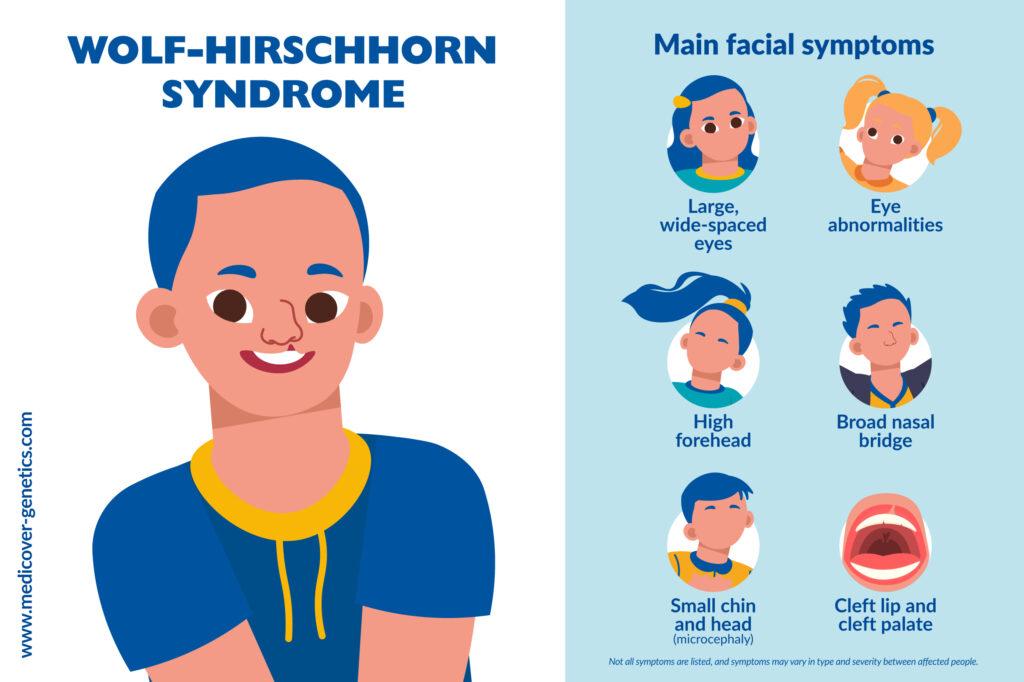
In many cases, a visual diagnosis is possible in a newborn or young infant.
Distinctive facial features include:
- Large, wide-spaced eyes
- A broad nasal bridge
- High forehead
- Arched eyebrows
- Eye problems: sloping eyelids, strabismus (misaligned eyes), iris colobomas (area of missing tissue)
- Small chin and head (microcephaly)
- Ear dysplasia
- Cleft lip and cleft palate
Other symptoms include:
- Developmental delay and intellectual disability
- Heart and kidney malformations
- Hypospadias (in boys)
Frequency
The frequency is estimated at 1:20,000 to 1:50,000. WHS occurs more often in females than in males (ratio 2:1).
Causes
WHS is caused by deletions of different sizes of the terminal short arm of chromosome 4 (4p16.3). Smaller deletions (up to 3.5 Mb) are associated with a milder presentation without malformations, medium deletions (5 to 18 Mb) are associated with classic presentation of WHS, and very large deletions (22-25 Mb) are associated with a very severe presentation that bears no similarity to WHS.
In classical WHS, the deletions are often detectable by conventional chromosomal analysis. Interstitial deletions with preserved subtelomeric regions also occur.
Inheritance
Between 85 and 90% cases of WHS are caused by a de novo (new) deletion that occurs spontaneously during embryonic development and can occur in individuals with no family history of WHS. The remaining 10-15% are due to structural chromosomal rearrangements, which may be present in the parents in a balanced form. Although a balanced translocation does not usually cause health issues, inheritance can cause it to become unbalanced, resulting in symptoms of the disorder.
Differential diagnosis
Syndromes with similar symptoms to WHS include Angelman, CHARGE, Cri-du-chat, Down, Seckel, Smith-Lemli-Opitz, Williams, Rett, Smith-Magenis syndromes.
References
Battaglia, Agatino et al. “Update on the clinical features and natural history of Wolf-Hirschhorn (4p-) syndrome: experience with 87 patients and recommendations for routine health supervision.” American journal of medical genetics. Part C, Seminars in medical genetics vol. 148C,4 (2008): 246-51. doi:10.1002/ajmg.c.30187Zollino et al. 2008, Am J Med Genet 148C:257. https://onlinelibrary.wiley.com/doi/10.1002/ajmg.c.30187.
Battaglia, A et al. “Wolf-Hirschhorn (4p-) syndrome.” Advances in pediatrics vol. 48 (2001): 75-113. Wright et al. 1998, Am J Med Genet 75:345. https://pubmed.ncbi.nlm.nih.gov/11480768/.
MedlinePlus [Internet]. Bethesda (MD): National Library of Medicine (US); [updated 2020 Jun 24]. Wolf-Hirschhorn Syndrome; [updated 2023 May 22]. Available from https://medlineplus.gov/genetics/condition/wolf-hirschhorn-syndrome
“Wolf-Hirschhorn Syndrome.” National Organization of Rare Diseases, 01 Oct. 2020 https://rarediseases.org/rare-diseases/wolf-hirschhorn-syndrome/
“Wolf-Hirschhorn syndrome.” Orphanet, updated May 2021, https://www.orpha.net/consor/cgi-bin/OC_Exp.php?lng=EN&Expert=280.